Author: admin
Day of Atonement

So today the Jewish religion celebrates the holiday of Yom Kippur. Yom Kippur for those who do not know is the most solemn and second only to the Sabbath as the holiest day of the year in Judaism. Its central themes are atonement and repentance. Jewish people traditionally observe this holy day with an approximate 25-hour period of fasting and intensive prayer, often spending most of the day in synagogue services. (This is referenced from Wikipedia.) Now, I was raised Jewish and consider myself to be a good Jew even though I may not go to temple today (or ever for that matter) or fast. To me, religion is more about how we treat each other than whether or not we have good attendance at temple/church or regardless of whether you stop eating for a day. I would also like to put a different wording to “atoning for sins or repentance.” I think the best way to look a this day is no different than how we should look at any day of our lives- as a constant learning process.
The best part of being a primary care physician, especially now that I have much more time to spend with patients, is that I really get to see people at their best and worst. I get to deeply learn about the human condition. And as a fellow human, I realize that we all have done and/or said things that we are not proud of. None of us are perfect nor will we ever be. Making mistakes is part of the learning process, and yes some are worse than others, but if we examine them and learn from them we can all grow and become a better person as a result of it. Right now in society there is a lot of rancor and venom being spread around. There is a lot of personal, internal unhappiness being projected or displaced onto others. When this happens, the cycle just repeats and repeats itself and the end result is no one ever heals- neither the person who was hurt nor the person that caused the hurt. We end up just hurting ourselves even more.
So take today- Yom Kippur- and make it and every day a “learning day”. Take the time to reflect about how you can change for the better and apologize to yourself for the mistakes you have made because until you forgive yourself, the people you have hurt won’t be able to feel the sincerity of the apology. I have always said we can only change ourselves and how we respond to people, not people. That change has to come from within. One of my favorite educators was Dr. Aaron Lazare MD who, may he rest in peace, was Dean of UMass Medical School when I was enrolled there. He was a psychiatrist and was one of the kindest people I have ever met. He wrote an incredible book called “On Apology” which spoke to how important an apology can be in life and in medicine. Here is a great quote from it:
“One of the most profound human interactions is the offering and accepting of apologies. Apologies have the power to heal humiliations and grudges, remove the desire for vengeance, and generate forgiveness on the part of the offended parties. For the offender, they can diminish the fear of retaliation and relieve the guilt and shame that can grip the mind with a persistence and tenacity that are hard to ignore.The result of the apology process, ideally, is the reconciliation and restoration of broken relationships.”
So realize we are all human….and we all screw up, but…we can apologize to ourselves so that we can heal from within and then…help others do the same.
Gut Yontiff
Why DPC IS The Answer!

Yesterday Dr. Edmond Weisbart wrote this article for Family Practice Management (http://www.aafp.org/fpm/2016/0900/p10.html#commenting) which we posted on our Facebook page last night. He basically gives reasons why he feels DPC is not a solution to our healthcare crisis. I took the liberty of writing the below rebuttal which I have since emailed to their editorial staff for publication as well as a medical blog called www.KevinMD.com. I truly hope you will read this, and if you agree with my arguments, help us DPC doctors across the country that are trying to fight for you, our patients, and speak up to everyone. Send letters to your congressmen and congresswomen. Send it to our governor. Share it on social media. WE- patients and doctors- need to fix this as people are paying more for healthcare than their mortgages and getting less and less in return.
September 14, 2016
I am writing this letter on behalf of my fellow DPC colleagues in response to the Opinion piece by Edmond S. Weisbart, MD, CPE, FAAFP from your September-October issue titled “Is Direct Primary Care the Solution to Our Health Care Crisis?” I will be so bold as to answer Dr. Weisbarts questions with an affirmative “yes” and will try to respond to each of his bullet points. For further reading that is excellently done and supported by fact please refer to Dr. Phil Eskews piece “In Defense of Primary Care.” (http://www.aafp.org/fpm/2016/0900/p12.html)
- DPCs exacerbate the growing physician shortage: No Dr. Weisbart, plain and simply our current system is exacerbating the shortage of physicians. People who choose to go into a primary care field want to care for patients and not be burdened with an excess amount of bureaucracy that prevents them from following their oath to provide said care. One could argue that many physicians taking administrative jobs, such as a CMO of a pharmacy company, could also be contributing to the “care” shortage and access problem. Maybe we should stop doing that? And having a panel size of 2,300 patient is a good thing? If our system continues down its current path our primary care will be nothing more than an Urgent Care clinic.
- DPC’s are essentially unregulated insurance, capitating physicians and removing vital protections: Where do i begin with this one? Insurance by definition is to protect people against major financial loss for major unexpected events i.e. life insurance, car insurance, home insurance etc. Primary care is not an insurable event, as everyone needs it and should have it. Primary care is actually highly affordable, but has been made expensive BECAUSE we insure it. And the difference between captivated plans from an HMO and DPC is that there is NO THIRD PARTY determining the capitated value for the primary care services. The sole value determinant is the actual patient. What a novel concept that we have completely failed to see since third party payers have stepped into primary care. You know? To help weed out those greedy PCP’s- compared to the affordable premiums people (many with chronic disease) are paying to to carry, only to have 3,000-6000 deductibles and zero transparency on pricing for outpatient services in the third party system. Plus, if providing your technical skills and knowledge for a set monthly fee is unethical or illegal, then why can lawyers, accountants, etc do this everyday? And as far as your HIPAA concern, in true DPC guess who has access to the patients file? me and the patient!. Thats it. No one else unless its the patients choice. Can’t get more private than that can you? If I do sell patients info to vendors I am pretty sure my state BORIM and the exodus of my patients will regulate me sufficiently thank you very much. No other third party or acronym needed for that.
- DPC relies on an erosion of medical benefits: Lets look at your first sentence. The under-utilization due to HDHPs is actually due to the fact that people have no access to transparent care due to this third party payment cartel we have abided by for decades. Secondly, the current system is THE “hardship to patients” because it is an over regulated Gordian knot. DPC is accessible, affordable, and transparent with discounted pricing on imaging, labs, and meds in most states- i.e. those that allow dispensing. We actually help patients navigate this nebulous system, save them money, and yes, get them to specialists when needed with less fragmentation of care through better communication with said specialists. The only thing that makes specialty referrals difficult is the insane red tape that already exists (ie HMO patients needing an “in-network PCP” as their gatekeeper. So much for being “locked in” to something right?) We also use services (at no extra cost to patient I may add) like RubiconMD that reduce a lot of unnecessary speciality referrals that the 8 minute visits in our current system exacerbate. Also, many specialists will also see patients for a cash price if uninsured or underinsured. Thirdly, as far as employer plans go, the employers allow their employees to choose their own physician. DPC is offered as an option, not a mandate. They still have insurance, albeit with copays and deductibles, if they choose to have a PCP in the 3rd party system. So that statement is completely erroneous.
- DPCs exacerbate disparities in care: I will simply ask this in rebuttal- instead of citing studies. Have you actually visited a DPC practice and spoken to the patients that are members? Yes, the wealthy can afford anything. But what about all of those people you mentioned in paragraph 2 of section 3? A 90 dollar lipid panel at a hospital based lab is better for a blue-collar patient/family than a 75-95 dollar a month primary care medical home with no copays/deductibles and a 6 dollar lipid panel? Do the math. And as far as your inference to “cherry picking” patients with chronic diseases such as diabetes- that is just completely false and presumptuous. If anything, myself and my colleagues have many patients whom the current system has completely failed. But again, maybe you should actually speak with some DPC patients? Many of us actually have Medicaid patients. Being “insured” does not equate to actually receiving “care.” I will even provide charity care for those truly in need. Maybe policymakers and Medicaid administrators would actually work with us to make the model more accessible to Medicaid patients? Maybe the government could give those patients a voucher card for DPC no different than they do for food stamps etc?
The bottom line Dr. Weisbart is that nothing we have done or continue to do with this top down approach to fix our broken healthcare system is working. We have many administrators, policymakers, and CEOs telling us how to fix this and plugging fingers in the dyke that is ready to collapse as people pay more for insurance than they do their mortgage! So why don’t we try listening to the doctors and patients that have become the blips in the matrix on how to fix this mess for a change? The best solution to a complex problem is often the simplest. Remember Occams razor?
Sincerely yours,
Jeffrey S Gold MD
Owner/CEO Gold Direct Care PC
123 Pleasant St Suite 105
Marblehead MA 01945
DPC Coalition Steering Committee Member
To Rent or To Buy: That is the Question
Depending on your age and income, and whether or not you are shopping for a car or a place to live, the answer to this question may vary. If you enjoy getting a new car every few years then leasing is clearly the way to go, but if you really like your car then buying would be the better choice. You will likely take better care of the car because you actually own it and have zero interest in having to make new car payments once it is fully paid. Same goes for renting an apartment versus buying a home. When you rent you are just simply handing over money to a landlord to live there. There are benefits to it such as maintenance and landscaping being covered, and if you only plan on being there a short time then renting is a great idea. However, if you are looking to have a long term or permanent place to live then buying is the way to go. You are investing in the roof over your head, your yard, and the upkeep of your property. In the long run it is a much better investment.
See chart from Trulia.com here for a visualization of how buying saves in the long run:
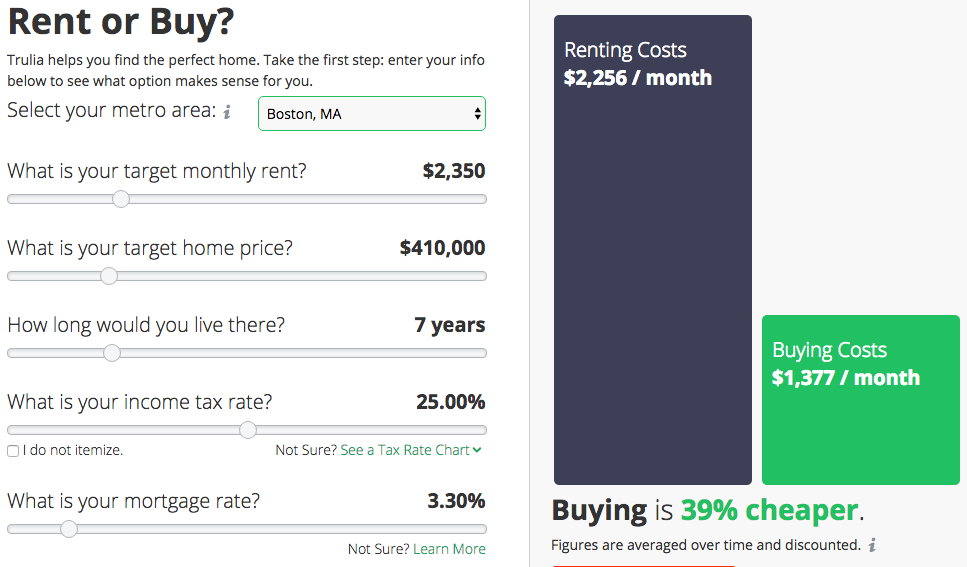
So I ask this question: why would anyone not want to do this for their healthcare, especially primary care which is the heart of medical care? This is nothing against the many great physicians that are employed and contracted with 3rd party payors, but when your primary care physician is being paid by a third party you are technically renting/leasing them. Maybe they will drop or be dropped by that third party? Maybe they will burn out and fade away which is happening all across the country? Maybe you will get lucky and just like the old days they will stay in one place and be contracted with your third party payor for years to come? Yes they took an oath to care for you which they do to the utmost of their abilities, but technically, given that they are being paid by their employer through your insurer they aren’t technically working for you
So what if you could own the relationship with your primary care physician and have them work only for you rather than leasing it? What if you- the patient/consumer- were the only party determining the worth and value of your doctor and the care that he/she provides instead of a third party that knows zilch about you as a person? What if you could have a mutually beneficial relationship with your personal physician based on respect and trust that exists in sickness and health? And what if you could have all of this investment for less than a coffee a day? After all isn’t your health, peace of mind, and wallet worth the investment? If the answers are yes then Direct Primary Care is here and here to stay. Lets take primary care and medicine back one doctor and patient at a time. You can rent DPC for a year and if you really like it- just like Chevy Chases’ rubber gloves in Fletch- it comes with an option to buy 🙂
Defragmentation of Care- PCP and Specialist Combined Visit ( A Medical Students Take)
When was the last time your PCP accompanied you to a specialist visit? Never? Same here. That’s actually not entirely surprising in today’s healthcare environment, given the demands placed on healthcare providers and primary care physicians in particular. But last week, I had the opportunity to be a part of such a visit.
I’m a medical student on my family medicine clerkship with Dr. Gold, and on his schedule this day was a cardiology visit for one of our 78 year-old patients. In the afternoon, we drove to meet her at the cardiologist’s office. She had recently had an episode of atrial fibrillation picked up by her pacemaker, and at this appointment, we would discuss the possibility of starting her on blood thinners. The cardiologist thoroughly explained the algorithms that guide decision-making for the treatment of new a-fib, along with the risks and benefits of blood thinners. He concluded by saying that, while he slightly favored starting the medication, he would leave the decision to our patient. As she took a moment to take in this information, her eyes began to well up. Amidst her tears, she explained that having to add yet another medication to her regimen or the thought of a stroke or going into a-fib again or bleeding from a fall was all too overwhelming to process.
The situation was complicated further by our patient’s chronic pain, which she experiences as a burning sensation across her lower chest. It has been treated with varying success for many years, and she was soon visiting a pain clinic for further assessment. So how was she to decide given these circumstances? The cardiologist offered expertise focused on giving her the best possible care for her cardiovascular health and went on to reassure her that the pain was not cardiac in origin. The presence of her primary care physician in addition, however, proved essential in helping her feel comfortable with her options. Primary care physicians are charged with taking care of the whole patient, a-fib, pain, tears and all. So when it became Dr. Gold’s turn to offer his input, he took a step back and considered her quality of life and her priorities. He helped her to sort through the risk calculators, EKG results and medication side effects to reveal what was really causing her the most distress each day and keeping her up at night. It was not her cardiac issues. It was her pain. Perhaps, he advised, we should address this issue first and then reconsider starting blood thinners in the future.
I would argue that any primary care physician would want this opportunity, the chance to sit down with his or her patient and another member of the healthcare team for one hour and determine what is really best for the patient at a given point in time. The problem is finding that hour amidst the multitude of patient visits, phone calls, notes, prior authorizations and EMR notifications. This time is what Dr. Gold offers his patients, and I believe that this single visit demonstrates how essential that time can be.
Tufts 3rd Year Medical Student
![]()
Employers and Direct Primary Care: A No-Brainer!

Not surprisingly, recent studies have shown a broad value proposition that links workplace health and well-being to favorable business performance. So why don’t more employers invest in programs that promote healthy employees? Expense is one glaring reason! Employers, both large and small, are being crushed by the rising cost of providing insurance benefits to their employees. Most employers address this growing cost by shifting it to their employees in the way of increased premiums, higher deductibles or higher co-pays. There is a cost effective solution and this solution is Direct Primary Care.
With Direct Primary Care, employers pay a fixed amount for all primary care services. This removes the guessing game on how much money will be spent on claims filed by employees. Direct Primary Care can be inserted into the overall health insurance plan offered to employees and ultimately control downstream costs. DPC, combined with an appropriate supplemental catastrophic plan, can save employers up to 40% on healthcare costs! This is all in accordance with the Affordable Care Act, so employers won’t get fined for non-compliance.
If saving money wasn’t enough to convince you, other perks for the employer include: decreased absenteeism, decreased workman’s comp claims, utilization of telemedicine to evaluate employees so they don’t leave early for doctors’ appointments or miss work altogether. Employees benefit too, as they receive same day appointments, a personal relationship with their physician, telemedicine/virtual visits, decreased out-of-pocket expenses, no more visits to urgent care centers.
Direct Primary Care physicians can be an employer’s most valuable ally as they search for ways to control healthcare costs, while simultaneously offering their employees the highest quality of care. Check out this article http://www.directdoctors.org/blog/direct-primary-care-a-solution-for-small-businesses to learn more.
If you are a business owner or know a business owner call us at 781-842-3961 to start saving money!
Our Obesity and Healthcare Epidemics: How They Go Hand in Hand

We all should know by now that we have a major obesity epidemic in this country. The best way to reverse this epidemic by controlling our weight and reducing our risk of diabetes, high blood pressure, and vascular disease is by eating real, unprocessed food. Doctors, nutritionists, and other healthcare providers often advise patients to shop the periphery when in a grocery store. Why? Because that is where the real food is. That’s where the produce, the real dairy products, fish, chicken, and meats are. Now, not all of these are truly healthy products which is beyond the scope of this post, but you catch my drift. If you shop the aisles and try to read the nutrition facts you will see my point. For example here is the nutrition info for Cheerios with Protein:
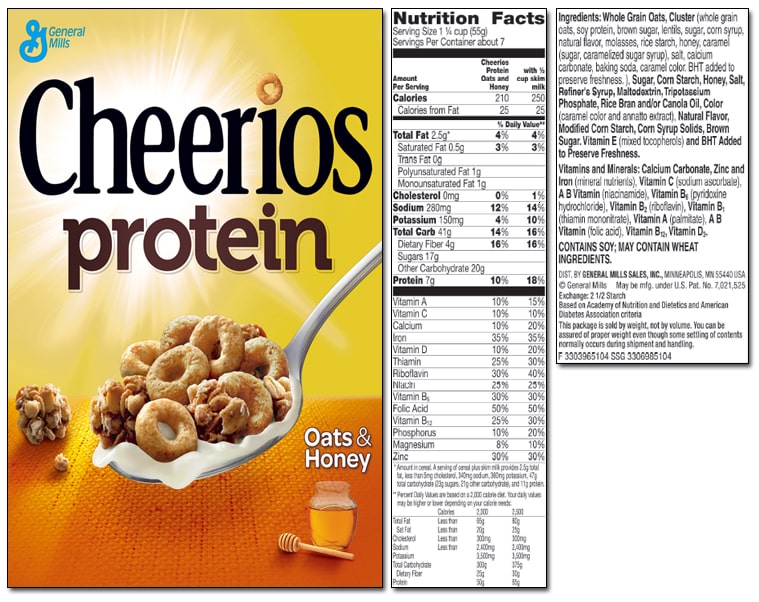
This may seem healthy on the front but look on the back and see that there are 41 grams of total carbohydrates and 17 grams of sugar! Even more interesting to point out is why is sugar one of the few items that does not have a daily percentage value next to it? Hmmmm…..Obscure. And look at the number of ingredients listed- most of which can not even be pronounced. All in all….not good and certainly not healthy. Real food is always the better option.
It is also recommended to try to cook and eat as home a much as possible to help you get or stay healthy. I am by no means a master chef but based on my experience whenever I have tried to make some complex recipe with a lengthy list of ingredients it has turned into a complete inedible mess. Ask my wife about the spice-rubbed pork tenderloin from Epicurious I tried to make a few years back…god awful. Yet, every time we use a recipe from Cooking Light it comes out great. There are fewer ingredients and fewer steps for one to screw up. It is simple, healthy and usually quite delicious. I’ll leave the complex recipes and dishes to the master chefs.
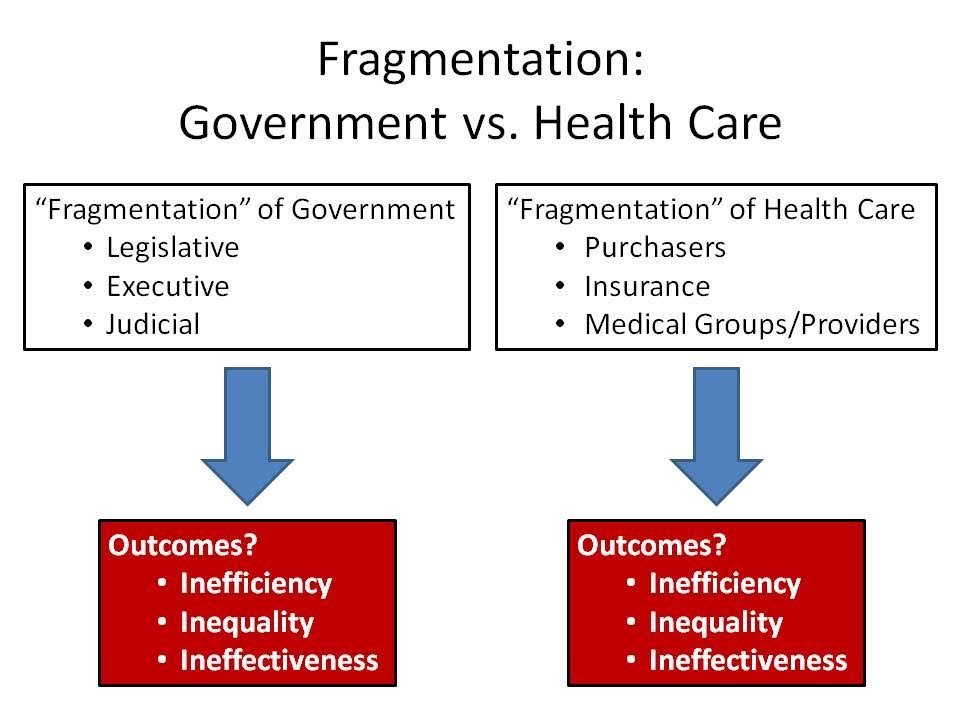
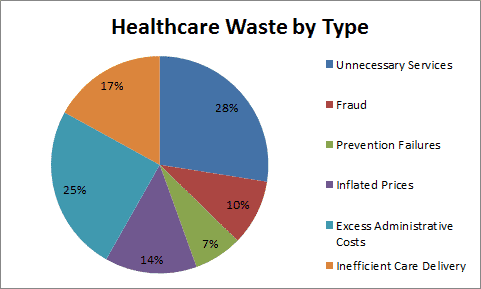
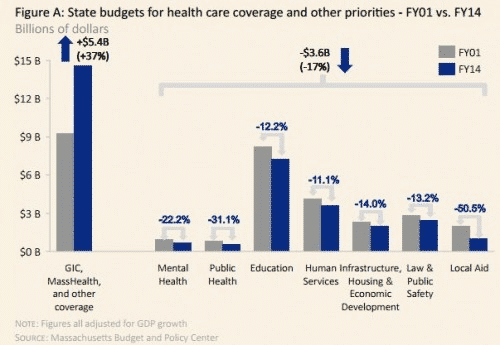
Hopefully by now you can see how this is going to tie in to our Healthcare Epidemic. Our system has become so bloated and complex with way too many needless ingredients and cooks in the kitchen that we can’t get out of our own way. See the proof here as our own state of MA spends 40% of the budget on Healthcare at the expense of other important needs:
While we keep adding layers of red tape and bureaucracy, as well as continuing to allow third parties (government and insurers) to set quality measures, create networks (i.e. doctors and hospitals whom you can and can’t use), and set nontransparent prices, the doctor/patient relationship- you know… where the actual care and medicine takes place- will continue to suffer. You will have less access, longer wait times, less time with your doctor, and more visits to an Urgent Care clinic. Is that really what people want for their healthcare?
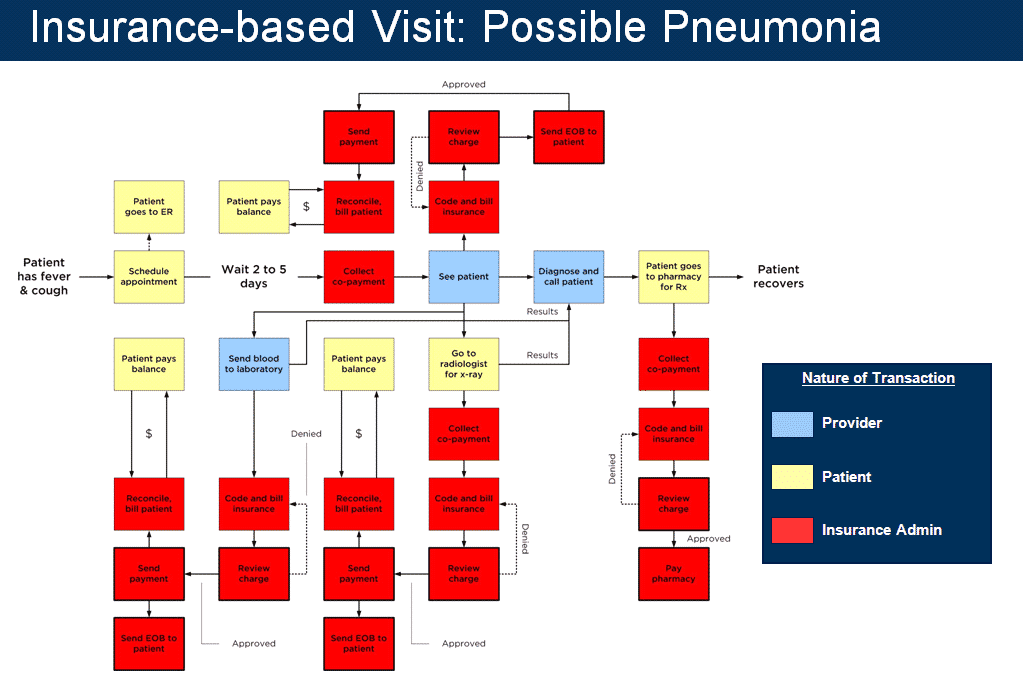
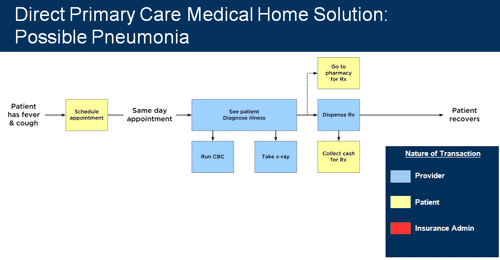
In conclusion, healthcare- especially primary care- does not have to be so expensive and complex if we just get rid of the wasteful ingredients. Let the patient, the actual consumer of the service/care, determine value and not a third party whose goal is profit and profit only. Let insurers be true insurers. Let government provide financial aid to those whom truly need it, but stop practicing medicine. Let the doctors practice medicine without layers of regulation and trust me, the bad ones will show themselves. In healthcare, just like with nutrition, the saying “less is more” could not be more appropriate. Just look at these these diagrams to see how DPC changes the recipe. *mic drop*
Why Are We Paying So Much Money For Health Insurance When We Still Can’t Afford Care?

The Boston Globe published an article on March 23, 2016 titled Even With Insurance, Mass Residents Often Can’t Afford Healthcare and I can’t even begin to explain how true this is. They really hit the nail on the head with this topic! Being a young adult, I can completely relate to what it’s like to not be able to afford health insurance. Not until last year did I really begin to understand how expensive health insurance really is. I started working for a big company which offered “the best” health insurance (no need to mention names). I was so excited to think I had this ‘top of the line’ health insurance. It was all great until of course, I made my first visit to the ER. With a very expensive co-pay, high deductible, and multiple bills later, I realized how unaffordable healthcare truly is. Just as this article states, having health insurance doesn’t necessarily mean you can afford care. I immediately noticed- yes, I finally have “great” health insurance, but does it even matter when I can’t afford to go to the doctor? With the statistics from the survey BCBS conducted, clearly I’m not the only one in the same boat. As mentioned in the article “43% of people said in 2015 health care and costs had caused problems for them and their families, including 19% who went without needed care as a result.” How crazy is it that almost 50% of the people surveyed have issues with health care costs?! That’s a huge percentage, which includes me, and possibly you too. We already have so many bills to pay and stress about, healthcare really shouldn’t be one of them. Another thing I noticed from the article are the comments being posted. So many people are complaining about this issue, yet they don’t want to do a single thing about it or, perhaps, they don’t know of other options out there. I think it’s time we start doing our research as healthcare consumers and see what other options we have out there!
This article really struck a chord with me, especially now knowing about Direct Primary Care and really understanding what it is. I wish I would have known about DPC earlier, or even know DPC was an option. Of course we do still need health insurance, but why not choose DPC for our primary care needs? This way we don’t have to deal with co-pays or high deductibles from our health insurance, not to mention getting more personalized care, appointments in a reasonable amount of time and honestly, a real connection with your doctor. Why wouldn’t you want a real connection with your doctor?! They are the ones who are dealing with a big part of your life; your health. The article from the Boston Globe should really relate to many of us, and also be an eye opener. With the results from the survey by BCBS, we can’t deny health insurance is way too expensive and we just aren’t receiving the best care for the amount we are paying. Instead, we end up with a huge headache because of very high bills and often poor to mediocre healthcare.
Written by Jessica Leon, Administrative Assistant; Gold Direct Care
Direct Primary Care: A Medical Students Perspective

As the end of our first year of medical school approached, we received our assignment for where we would complete our primary care apprenticeship for the following year. After the countless hours of studying in isolation, we would finally be fully emerged in a setting to interact with patients and be able to put a face to the multitude of diseases and medications that we spent learning in the prior months. Before our first day at Gold Direct Care, we only had our own experiences as patients as well as the opinions- both positive and negative- from doctors and upperclassman to guide our perceptions of what it would be like to be a primary care physician. Among opinions of fellow classmates, rarely would we hear, “I want to be a primary care doctor.” As for physicians, a compilation of their opinions illustrated the picture of the primary care physician as a half assembly line worker and half paper pusher. Furthermore, in order to provide the best possible “patient centered care,” there were certain rules set by administrators and insurers. Everyday you will see 26 patients. For each appointment, you have 15 minutes to obtain an accurate and complete history and physical exam, strengthen the doctor-patient relationship by establishing rapport and find the time to teach medical students and residents. And the reward for successfully juggling all of these tasks is a stack of endless paperwork waiting to be completed.
As we walked through the doors on our first day, the dreaded barriers that we envisioned were nowhere to be found. In fact, we quickly learned that Direct Primary Care (DPC) and Dr. Gold operated by a different set of rules. There was no time limit for each appointment and the length was determined by no one other than the patient. Thus, there was not only more than sufficient time to address all of the patient’s wants and needs, but also to establish a strong rapport in order to strengthen the relationship between the two most important people in healthcare, the doctor and the patient. Since Dr. Gold never had to worry about a stack of paperwork, he was able to reallocate that time towards teaching. Specifically, we had the opportunity to interview every patient, perform a detailed physical exam and properly document the encounter while being supervised and guided by Dr. Gold in order to maximize every learning opportunity. While these may just seem to be unique characteristics of Dr. Gold, it is the environment created by DPC that allows great people like Dr. Gold to be great doctors to their patients, as well as great teachers to their students. After our experiences working at Gold Direct Care, the negative picture of primary care that we originally envisioned had transformed into one that any current or future doctor would desire.
With a desperate need to attract more medical students into primary care, students are still reluctant to pursue careers in primary care. Dr. Gold and DPC offer solutions to this problem. Doctors can practice medicine the way it ought to be practiced, which is solely focused on the doctor and the patient. Instead of working for an insurance agency, you get to work for your patients, who will ultimately determine your value. No more paper pushing, no more assembly line, just the doctor and the patient working together to improve health outcomes- a recipe that will make primary care a very attractable career path for medical students once again. After arranging an information session for Dr. Gold to share the benefits of DPC with our class, it was quite evident that we were not alone with our enthusiasm regarding DPC. In fact, shortly after its conclusion, a fellow student sent us a text “Guys, I think I want to do primary care now!”
Thank you to Dr. Gold and Meghann for this incredible learning experience. Everything you taught has been invaluable and will help shape our future careers in medicine. Also we would like to thank all of Dr. Gold’s patients for allowing us to learn through hands on experience and giving us advice that will help improve our abilities as future physicians.
Michael Held & Douglas Rodgers
Tufts Medical School Class of 2018
A Win For Gold Direct Care and DPC in MA

![]()
Direct Primary Care is written into the Affordable Care Act as an approved method of receiving primary care as long as it is combined with a catastrophic insurance plan. (Isn’t that how insurance is supposed to work? But I digress.) The ACA clearly defines that DPC is not “insurance” and purchasing a DPC membership alone does not meet the standards of being “insured.” It is required to purchase at least a high deductible insurance plan along with it to be qualified under the ACA. See great article on this here: DPC Clause in the Affordable Care Act
However, on the State level, many legislators, policy makers, and Department of Insurance commissioners want to claim that DPC is the “business of insurance” and should have to pay licensing and regulatory fees. In other words, paying a reasonable monthly fee for all your primary care needs should be regulated no different than Blue Cross Blue Shield, Harvard Pilgrim, etc etc. Having to pay fees of this magnitude would clearly put a small DPC practice like us out of business. We are not “insurance”. We are a primary care medical practice that chooses to work solely for our patients- not third parties- and therefore be compensated by our patients for what we believe is a reasonable monthly fee. About 15 states in the US have now passed legislation stating this as law. Massachusetts is not one of them and has yet to introduce a bill that by stating such protects us and our patients who choose us. We, along with three new DPC practices in MA, are tirelessly working on getting our legislators to listen to us and sponsor a bill.
As the first DPC practice in MA we were contacted by the Massachusetts Department of Insurance when we first opened in January 2015. With our legal counsel we have met with them and corresponded with them on this issue. It has been months of waiting and practicing medicine in an unclear regulatory environment. This weekend, much to my delight, I was contacted by my attorney with a letter from the DOI that has given us the green light to continue practicing medicine without 3rd party interference. (The letter is attached below a sit is a public document.) We are very thankful to Commissioner Daniel Judson and Deputy Commissioner Kevin Beagan for their understanding that what we are trying to do is solely for the benefit of the people of Massachusetts and the primary care doctors who want to care for them in a manner that echoes the “olden days of medicine.” Hopefully there are better days ahead for healthcare in Massachusetts. (more…)
It Was the Best of Days and the Worst of Days

Last Wednesday, January 6 2016, was a day I will not forget any time soon. It was a day that showed me the worst of our healthcare system but also the best. The week prior, a new patient enrolled with us online. His name was not one that was familiar to me. We scheduled him for a full checkup the next week. Patient X is a 29 year old male chef that found me online because he had no health insurance and was looking for an affordable entryway into our healthcare system. He had applied for Medicaid but was waiting on confirmation. He is a hard working, honest guy that could not afford to purchase any of the “affordable Obamacare plans” on the exchange. Luckily, he did qualify for subsidies to get MassHealth but he was not confirmed at the time of our visit. For this, I will thank Obamacare. It is not bad in every way.
After my nurse put him in the exam room and got some information on him she came back to my office to tell me about the multitude of symptoms he had been having for the past 4-6 months. These symptoms had worsened over the past few weeks and finally prevented him from working. These symptoms included left sided headache with blurred vision in his left eye, bilateral hip pain, back pain, some weight loss, and an enlarging lump in his testicle which he attributed to an enlarging benign cyst that was diagnosed by another physician years prior. Clearly he was anxious and you know what? So was I.
As I entered the exam room I was greeted by a tall, slender and very personable young guy. We walked through the details of his symptoms and the time course. I encouraged him to relax and take his time since with Direct Care there is happily no more rushing through the mill. Needless to say his story was very concerning to me and it was amazing to me that this guy was able to perform labor up until two weeks prior, especially since the pain was keeping him up at night. After his history, I conducted a thorough head to toe exam. He only had minimal neurologic findings. When he was lying down so I could examine his abdomen I could see a large left sided mass in his groin under his shorts. Sadly, all the worst-case scenarios that were running through my head were now close to being confirmed. As he stood up and lowered his shorts I was presented with the culprit- a large left sided testicular mass with swollen nodes in his groin- i.e. it had already spread and now I was concerned that all his other symptoms were manifestations of the same. This was not an easy conversation to have but I sat with him and relayed my concerns.
So the first worst part of the day was seeing this guy suffer with awful symptoms for so long without engaging our system. Was it fear of illness that kept him away? Fear of cost? Denial? Truthfully it was probably a combination of all of the above. The hard part for me was seeing the regret on his face. I tried to reassure him that what is done is done and we can not go back in time, but that we need to deal with the here and now and move forward. And so we did.
So now for the best part of the day. Within 20 minutes our wonderful insurance broker, George Claassen, came over to the office to meet with Patient X and get his insurance confirmed, as I knew he would be heading for extensive and expensive treatment- the stuff for which insurance should be used. While he met with George, I was on the phone with a great local urologist who agreed to see the patient that afternoon and was willing to do a cash price for him if needed. Following his visit the patient called me and told me it was advised that he would need CAT scans the next day prior to urgent surgery that was scheduled for Friday AM. Thank god we got him on insurance right?
That is until he told me that his new Medicaid plan would not cover the CAT scans- CAT scans ordered by a specialist with years of experience that is CONTRACTED with MassHealth!- the second worst part of the day. He was told by the schedulers at the hospital that the order needed to come from a MassHealth PCP! What planet am I on? A specialist nor an MD who diagnosed his condition can’t order an outpatient scan because of what?… Bureaucracy of course. I will not bore you with more details as the situation ended up working out and he got his scans the next day- which sadly showed spread of disease to bone, brain, nodes etc- and he had surgery last Friday. He is now in the hospital with a long arduous road ahead while he awaits chemotherapy. His pain is under better control and all we can do now is hope that his strong constitution and will to get better will guide him to being fully cured. But did he really need the two hours of aggravation after being told he had bad disease?
So like I said…it was the best of days and the worst of days all wrapped into one. It glaringly showed the positives and negatives of our system in the USA. All I hope for is the “best of days” when I can say that Direct Primary Care- for 50$ a month- saved the life of a really nice, polite, hardworking, appreciative, 29 year old year guy. It is an honor to be his doctor.
Disclaimer: this was written with the patients consent and he approved its content prior to posting.

